泌尿时讯 发表时间:2026/5/24 21:52:23
编者按:对于局限性前列腺癌,根治性放疗是重要手段,其疗效与手术相当,尤其适合高龄或无法耐受手术的患者。然而,放疗面临抗性困境,尤其部分肿瘤细胞因DNA损伤修复能力增强、缺氧微环境、肿瘤微环境支持及癌干细胞富集等机制而产生放射抵抗,影响治疗效果。近期,有学者总结了局限性前列腺癌的放疗耐药机制、生物标志物探索及未来方向,肿瘤瞭望-泌尿时讯特别整理,以飨读者。
亮点抢先看:
1
局限性前列腺癌放疗失败的主要原因是生物学抵抗,而非剂量输送的物理限制。
2
放疗抵抗源于多种内源性和获得性过程,这些过程在肿瘤及其微环境通路中相互作用。
3
需要预测放疗敏感性的生物标志物,以实现放疗方案选择和强度的个体化。
前列腺癌是全球男性最常见的恶性肿瘤之一,也是48个国家癌症死亡的首要原因。在美国,约有三分之一的局限性前列腺癌患者接受放射治疗而非手术,虽然长期癌症控制效果相似,但功能预后却有所不同。尽管在治疗计划和影像引导方面取得了进展,但仍有三分之一的患者在放射治疗后出现疾病复发,这凸显了更好地进行患者分层的必要性。
局部复发多见于原发灶区域,这提示具有放射抵抗性的肿瘤细胞是复发的主要生物学基础。尽管剂量递增(如RTOG-0126试验)和近距离放疗加强(如ASCENDE-RT试验)可提升生化控制率,但均未能完全杜绝局部复发。即使在少数剂量强化可改善总生存的研究中(例如GETUG-AFU-18试验),复发依然常见。综上,单纯依靠剂量强化似乎难以完全克服肿瘤的放射抵抗性。要实现实质性进展,未来策略需更多着眼于肿瘤本身的生物学特性,并针对其进行靶向干预。
目前,前列腺癌的临床预后主要依据TNM分期、Gleason评分和前列腺特异性抗原(PSA)水平进行分层。然而,这些指标无法有效评估肿瘤对放射治疗的敏感性。由于内在及获得性耐药途径的存在,肿瘤具有高度的生物学异质性,这也解释了为何临床特征相似的患者,在接受相同放疗方案后仍可出现截然不同的疗效。
因此,若要进一步提高放疗控制率,关键需在分子层面阐明放射耐药的相关生物学通路,并将其转化为可应用的分子标志物(如基因特征),从而在治疗前识别出放射敏感性不同的肿瘤,实现个体化治疗指导。
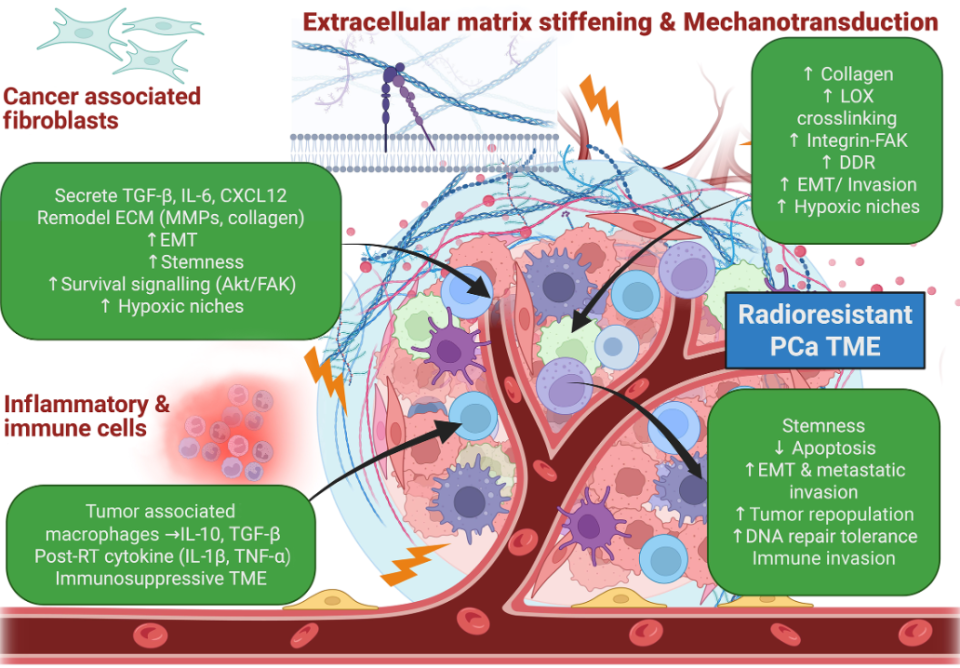
前列腺癌的放射抗性源于内在和获得性两类机制。内在抗性由肿瘤固有的生物学特征决定,例如活跃的DNA损伤修复(DDR)机制、特定的基因组改变,以及由雄激素受体信号通路驱动的修复功能。而获得性抗性则是在治疗中逐渐形成的,分次放疗的筛选压力使那些具有更强DNA修复、缺氧适应、干细胞特性或基质支持能力的肿瘤克隆得以存活和扩增。这些相互交织的通路,共同维持了一个具有放射抗性的肿瘤细胞群体,从而解释了临床上常见的、即便经过放疗仍持续存在的局部复发模式(图1)。
图1 导致前列腺癌放疗抗性的关键生物学通路
DDR能力是决定肿瘤固有放疗抵抗的关键因素之一。同源重组或非同源末端连接等修复通路活性较高的肿瘤,能够更有效地修复放疗引起的DNA双链断裂,从而在辐射后存活。其中,RAD51表达上调及ATM检查点信号通路的增强,可加速DNA损伤的修复进程,促进肿瘤细胞在放疗后存活。值得注意的是,雄激素受体信号通路能直接调控多个DDR相关基因的表达,从而强化这一修复机制。临床观察也支持这一关联:更彻底的雄激素受体抑制可增加肿瘤的放射敏感性;而像HSD3B1(1245C)这类基因变异,能够维持肿瘤内部的二氢睾酮水平,从而持续激活AR信号并进一步增强DDR能力,最终导致放疗抗性上升。
低氧是导致放疗抗性的另一明确机制。氧气是修复辐射所致DNA损伤的必要条件,处于低氧状态的肿瘤细胞,其放射抵抗性可达常氧细胞的2~3倍。这种缺氧的微环境有助于维持一类增殖相对缓慢、具有干细胞特性的肿瘤细胞群体,这类细胞通常对常规治疗反应较差。此外,缺氧可激活低氧诱导因子-1α依赖的细胞存活与DNA修复通路,从而进一步增强肿瘤对辐射损伤的抵抗能力。
肿瘤微环境是调节肿瘤对放疗反应的重要因子(图2)。在前列腺癌中,癌相关成纤维细胞可驱动形成一种致密且胶原丰富的细胞外基质。胶原交联的增加能增强整合素-黏着斑激酶信号传导,进而促进肿瘤细胞存活、DNA损伤耐受以及上皮-间质转化。此外,癌相关成纤维细胞还能通过持续重塑细胞外基质,并分泌转化生长因子-β、白细胞介素-6、CXCL12等因子,进一步支持上皮-间质转化、肿瘤干细胞特性的维持及疾病进展。上述过程共同导致基质纤维化与血管功能不良,阻碍药物与氧气扩散,加剧肿瘤内部缺氧,最终形成一个有利于维持肿瘤放射抵抗的微环境。
图2 前列腺癌肿瘤微环境是放疗抗性的驱动因素
前列腺癌的放疗抗性还涉及癌症干细胞富集、代谢适应及免疫抑制等多种生物学过程。目前,DNA损伤修复效率、雄激素受体信号通路、缺氧微环境以及癌相关成纤维细胞-细胞外基质重塑,被认为是该疾病中的主要耐药机制。这些通路共同构成了治疗失败的关键生物学基础,也为开发具有前列腺癌特异性的放射敏感性生物标志物提供了重要靶点与理论依据。
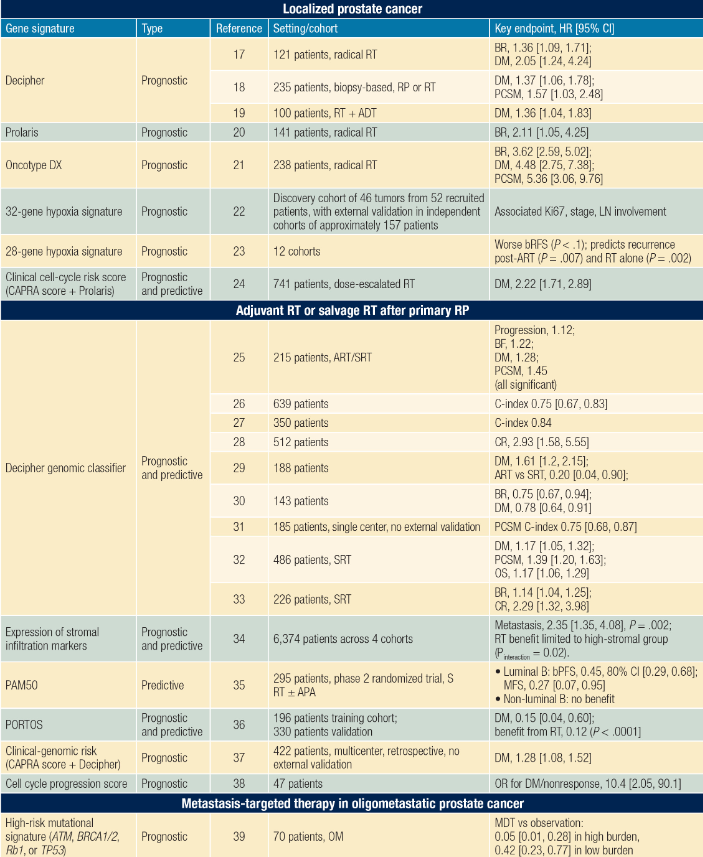
基因表达生物标志物通过检测特定基因组,可量化肿瘤的生物学特征。在前列腺癌领域,已有多种基因组特征被开发用于预后评估,但目前尚无可直接测量肿瘤内在放射敏感性、或可靠预测放疗获益的工具。
其中,Decipher(包含22个基因)是当前应用最广泛的预后基因组分类器。其评分较高者,可能从辅助或早期挽救性放疗中获益更多,但这主要反映的是患者本有的高进展风险,而非肿瘤对放射的内在敏感性。类似地,NRG-GU006研究发现,转录亚型可用于预测在挽救性放疗基础上加用阿帕他胺的疗效,这同样指向治疗反应的预测,而非纯粹的放射敏感性评估。此外,低氧相关基因特征能够反映肿瘤内与缺氧相关的耐药生物学,并在部分队列中显示出与放疗结局的相关性。然而,在联合雄激素剥夺治疗的高危患者中,其预后价值有限,这凸显了不同治疗背景下生物标志物表现的差异。
总体而言,目前能直接预测放疗益处的检测方法极少。现有标志物所提示的信号,更多反映的是总体预后或对联合治疗的反应差异,而非内在放射敏感性本身,且相关证据大多来源于回顾性分析。
放射敏感性评估工具虽然具有跨癌种应用的潜力,但其在前列腺癌中的有效性尚未得到充分验证。放射敏感性指数(RSI)是一种基于10个基因的模型,其通过评估细胞在2 Gy辐射剂量下的体外存活分数来量化肿瘤的固有放射敏感性。其衍生方法“基因组校正辐射剂量”则将RSI与放疗剂量相结合,曾在一些混合瘤种的队列中显示出预后预测价值。然而,这些方法在前列腺癌中缺乏生物学和临床上的稳健性。一方面,其基于2 Gy体外存活分数的模型与临床实际的相关性不足;另一方面,该模型在不同数据集中的表现波动较大。截至目前,尚无前瞻性或独立的外部验证研究能够证明,RSI或基因组校正辐射剂量可以可靠地预测前列腺癌患者的预后,或用于指导个体化的放疗剂量调整。
新兴生物标志物日益提示,肿瘤微环境是决定前列腺癌生物学行为及放疗反应的关键因素。例如,基质浸润程度评分与患者转移风险相关,并能识别出可能从术后放疗中获益更大的群体。其中,细胞外基质-癌相关成纤维细胞相关指标具有稳定性高、可在常规活检组织中检测的优势,使其成为基于肿瘤微环境的理想生物标志物候选者。分子影像学则提供了另一维度的生物学信息。前列腺特异性膜抗原-PET提高了隐匿性病灶的检出率,支持建立分子影像分期体系。多参数MRI可捕捉前列腺内的肿瘤异质性,其中功能成像序列(如反映缺氧状态的指标)正受到越来越多的关注。尽管这些进展共同推动着基于生物学信息进行更精细的风险分层,但目前尚无成熟的生物标志物能够直接定义肿瘤的内在放射敏感性。
目前,局部前列腺癌的治疗进步依赖于将肿瘤生物学特征有效整合到临床决策中。现有的预后工具虽可对风险进行分层,但尚无法准确预测患者能否从放疗中获益、是否更适合手术,或是否需要强化治疗。若未来能建立预测性的放射敏感性特征,则可将肿瘤区分为放射敏感型与固有耐药型。对放射敏感的肿瘤,或许可采用标准甚至减量的放疗,并尽可能减少或免去雄激素剥夺治疗;而对放射耐药的肿瘤,则可能需要考虑手术,或采用生物学强化的放疗策略,例如联合使用雄激素受体靶向药物。此类预测特征必须在常规诊断组织中即可检测,并需经过前瞻性、生物学驱动的前瞻试验加以验证,方能真正应用于临床。
综上,以放射敏感性、缺氧状态、基质生物学及雄激素受体信号通路为核心构建的评估框架,为实现生物学指导的精准放疗提供了合理路径,有望实现更持久的疾病控制。
参考文献:
1. Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209-249.
2. Scherzer ND, DiBiase ZS, Srivastav SK, Thomas R, DiBiase SJ. Regional differences in the treatment of localized prostate cancer: an analysis of surgery and radiation utilization in the United States. Adv Radiat Oncol. 2019;4(2):331-336.
3. Shore ND, Moul JW, Pienta KJ, Czernin J, King MT, Freedland SJ. Biochemical recurrence in patients with prostate cancer after primary definitive therapy: treatment based on risk stratification. Prostate Cancer Prostatic Dis. 2024;27(2):192-201.
4. Arrayeh E, Westphalen AC, Kurhanewicz J, et al. Does local recurrence of prostate cancer after radiation therapy occur at the site of primary tumor? Results of a longitudinal MRI and MRSI study. Int J Radiat Oncol Biol Phys. 2012;82(5):e787-e793.
5. Michalski JM, Moughan J, Purdy J, et al. Effect of standard vs dose-escalated radiation therapy for patients with intermediate-risk prostate cancer: the NRG oncology RTOG 0126 randomized clinical trial. JAMA Oncol. 2018;4(6):e180039.
6. Rodda S, Tyldesley S, Morris WJ, et al. ASCENDE-RT: an analysis of treatment-related morbidity for a randomized trial comparing a low-dose-rate brachytherapy boost with a dose-escalated external beam boost for high- and intermediate-risk prostate cancer. Int J Radiat Oncol Biol Phys. 2017;98(2):286-295.
7. Hennequin C, Sargos P, Roca L, et al; French Genito-Urinary Tumours Study Group (GETUG). Long-term results of dose escalation (80 vs 70 Gy) combined with long-term androgen deprivation in high-risk prostate cancers: GETUG-AFU 18 randomized trial. J Clin Oncol. 2024;42:4s (suppl; LBA259).
8. Boutros PC, Fraser M, Harding NJ, et al. Spatial genomic heterogeneity within localized, multifocal prostate cancer. Nat Genet. 2015;47(7):736-745.
9. Chaiswing L, Weiss HL, Jayswal RD, Clair DKS, Kyprianou N. Profiles of radioresistance mechanisms in prostate cancer. Crit Rev Oncog. 2018;23(1-2):39-67.
10. Fraser M, Sabelnykova VY, Yamaguchi TN, et al. Genomic hallmarks of localized, non-indolent prostate cancer. Nature. 2017;541(7637):359-364.
11. Polkinghorn WR, Parker JS, Lee MX, et al. Androgen receptor signaling regulates DNA repair in prostate cancers. Cancer Discov. 2013;3(11):1245-1253.
12. Sabharwal N, Sharifi N. HSD3B1 genotypes conferring adrenal-restrictive and adrenal-permissive phenotypes in prostate cancer and beyond. Endocrinology. 2019;160(9):2180-2188.
13. Brown JM, Wilson WR. Exploiting tumour hypoxia in cancer treatment. Nat Rev Cancer. 2004;4(6):437-447.
14. Cairns RA, Harris IS, Mak TW. Regulation of cancer cell metabolism. Nat Rev Cancer. 2011;11(2):85-95.
15. Popova NV, Jücker M. The functional role of extracellular matrix proteins in cancer. Cancers (Basel). 2022;14(1):238.
16. Yang D, Liu J, Qian H, Zhuang Q. Cancer-associated fibroblasts: from basic science to anticancer therapy. Exp Mol Med. 2023;55(7):1322-1332.
17. Berlin A, Murgic J, Hosni A, et al. Genomic classifier for guiding treatment of intermediate-risk prostate cancers to dose-escalated image guided radiation therapy without hormone therapy. Int J Radiat Oncol Biol Phys. 2019;103(1):84-91.
18. Nguyen PL, Haddad Z, Ross AE, et al. Ability of a genomic classifier to predict metastasis and prostate cancer-specific mortality after radiation or surgery based on needle biopsy specimens. Eur Urol. 2017;72(5):845-852.
19. Nguyen PL, Martin NE, Choeurng V, et al. Utilization of biopsy-based genomic classifier to predict distant metastasis after definitive radiation and short-course ADT for intermediate and high-risk prostate cancer. Prostate Cancer Prostatic Dis. 2017;20(2):186-192.
20. Freedland SJ, Gerber L, Reid J, et al. Prognostic utility of cell cycle progression score in men with prostate cancer after primary external beam radiation therapy. Int J Radiat Oncol Biol Phys. 2013;86(5):848-853.
21. Janes JL, Boyer MJ, Bennett JP, et al. The 17-gene genomic prostate score test is prognostic for outcomes after primary external beam radiation therapy in men with clinically localized prostate cancer. Int J Radiat Oncol Biol Phys. 2023;115(1):120-131.
22. Ragnum HB, Vlatkovic L, Lie AK, et al. The tumour hypoxia marker pimonidazole reflects a transcriptional programme associated with aggressive prostate cancer. Br J Cancer. 2015;112(2):382-390.
23. Yang L, Roberts D, Takhar M, et al. Development and validation of a 28-gene hypoxia-related prognostic signature for localized prostate cancer. EBioMedicine. 2018;31:182-189.
24. Tward J, Lenz L, Flake DD II, et al. The clinical cell-cycle risk (CCR) score is associated with metastasis after radiation therapy and provides guidance on when to forgo combined androgen deprivation therapy with dose-escalated radiation. Int J Radiat Oncol Biol Phys. 2022;113(1):66-76.
25. Spratt DE, Liu VYT, Michalski J, et al. Genomic classifier performance in intermediate-risk prostate cancer: results from NRG oncology/RTOG 0126 randomized phase 3 trial. Int J Radiat Oncol Biol Phys. 2023;117(2):370-377.
26. Erho N, Crisan A, Vergara IA, et al. Discovery and validation of a prostate cancer genomic classifier that predicts early metastasis following radical prostatectomy. PLoS One. 2013;8(6):e66855.
27. Lee DI, Shahait M, Dalela D, et al. External validation of genomic classifier-based risk-stratification tool to identify candidates for adjuvant radiation therapy in patients with prostate cancer. World J Urol. 2021;39(9):3217-3222.
28. Dalela D, Santiago-Jiménez M, Yousefi K, et al. Genomic classifier augments the role of pathological features in identifying optimal candidates for adjuvant radiation therapy in patients with prostate cancer: development and internal validation of a multivariable prognostic model. J Clin Oncol. 2017;35(18):1982-1990.
29. Den RB, Yousefi K, Trabulsi EJ, et al. Genomic classifier identifies men with adverse pathology after radical prostatectomy who benefit from adjuvant radiation therapy. J Clin Oncol. 2015;33(8):944-951.
30. Den RB, Feng FY, Showalter TN, et al. Genomic prostate cancer classifier predicts biochemical failure and metastases in patients after postoperative radiation therapy. Int J Radiat Oncol Biol Phys. 2014;89(5):1038-1046.
31. Cooperberg MR, Davicioni E, Crisan A, Jenkins RB, Ghadessi M, Karnes RJ. Combined value of validated clinical and genomic risk stratification tools for predicting prostate cancer mortality in a high-risk prostatectomy cohort. Eur Urol. 2015;67(2):326-333.
32. Feng FY, Huang HC, Spratt DE, et al. Validation of a 22-gene genomic classifier in patients with recurrent prostate cancer: an ancillary study of the NRG/RTOG 9601 randomized clinical trial. JAMA Oncol. 2021;7(4):544-552.
33. Dal Pra A, Ghadjar P, Hayoz S, et al. Validation of the Decipher genomic classifier in patients receiving salvage radiotherapy without hormone therapy after radical prostatectomy – an ancillary study of the SAKK 09/10 randomized clinical trial. Ann Oncol. 2022;33(9):950-958.
34. Mahal BA, Alshalalfa M, Zhao SG, et al. Genomic and clinical characterization of stromal infiltration markers in prostate cancer. Cancer. 2020;126(7):1407-1412.
35. Spratt DE, Karrison TG, Sandler HM, et al. A double-blinded placebo-controlled biomarker stratified randomized trial of apalutamide (APA) and radiotherapy for recurrent prostate cancer (NRG GU006, BALANCE trial). Int J Radiat Oncol Biol Phys. 2025;123(4):1197-1198.
36. Zhao SG, Chang SL, Spratt DE, et al. Development and validation of a 24-gene predictor of response to postoperative radiotherapy in prostate cancer: a matched, retrospective analysis. Lancet Oncol. 2016;17(11):1612-1620.
37. Ross AE, Den RB, Yousefi K, et al. Efficacy of post-operative radiation in a prostatectomy cohort adjusted for clinical and genomic risk. Prostate Cancer Prostatic Dis. 2016;19(3):277-282.
38. Koch MO, Cho JS, Kaimakliotis HZ, et al. Use of the cell cycle progression (CCP) score for predicting systemic disease and response to radiation of biochemical recurrence. Cancer Biomark. 2016;17(1):83-88.
39. Deek MP, Van der Eecken K, Sutera P, et al. Long-term outcomes and genetic predictors of response to metastasis-directed therapy versus observation in oligometastatic prostate cancer: analysis of STOMP and ORIOLE trials. J Clin Oncol. 2022;40(29):3377-3382.
40. Reardon MD, Bibby BAS, Thiruthaneeswaran N, et al. Hypoxia-associated gene signatures are not prognostic in high-risk localized prostate cancers undergoing androgen deprivation therapy with radiation therapy. Int J Radiat Oncol Biol Phys. 2025;121(3):752-760.
41. Guerrero Quiles C, Fahy S, Bartak M, et al. Radiation-induced extracellular matrix remodelling drives prognosis and predicts radiotherapy response in muscle-invasive bladder cancer. Front Oncol. 2025;15:1616943.
42. Torres-Roca JF, Eschrich S, Zhao H, et al. Prediction of radiation sensitivity using a gene expression classifier. Cancer Res. 2005;65(16):7169-7176.
43. Scott JG, Sedor G, Ellsworth P, et al. Pan-cancer prediction of radiotherapy benefit using genomic-adjusted radiation dose (GARD): a cohort-based pooled analysis. Lancet Oncol. 2021;22(9):1221-1229.
44. Mistry HB. Radiosensitivity index is not fit to be used for dose adjustments: a pan-cancer analysis. Clin Oncol (R Coll Radiol). 2023;35(9):565-570.
45. Eiber M, Herrmann K, Calais J, et al. Prostate cancer molecular imaging standardized evaluation (PROMISE): proposed miTNM classification for the interpretation of PSMA-ligand PET/CT. J Nucl Med. 2018;59(3):469-478.
46. Zhong J, Frood R, McWilliam A, et al. Prediction of prostate tumour hypoxia using pre-treatment MRI-derived radiomics: preliminary findings. Radiol Med. 2023;128(6):765-774.
(来源:《肿瘤瞭望-泌尿时讯》编辑部)
声 明
凡署名原创的文章版权属《肿瘤瞭望-泌尿时讯》所有,欢迎分享、转载(开白可后台留言)。本文仅供医疗卫生专业人士了解最新医药资讯参考使用,不代表本平台观点。该等信息不能以任何方式取代专业的医疗指导,也不应被视为诊疗建议,如果该信息被用于资讯以外的目的,本站及作者不承担相关责任。
温馨提示
添加小助手请备注“泌尿”